Skip to content
Menu
Home
Blog
About
Privacy Policy
Terms of Use
Posters
Eye Health
Discussion
Vision Therapy
Notes
Flashcards
Be a Member
Login
Register
Optometry Notes
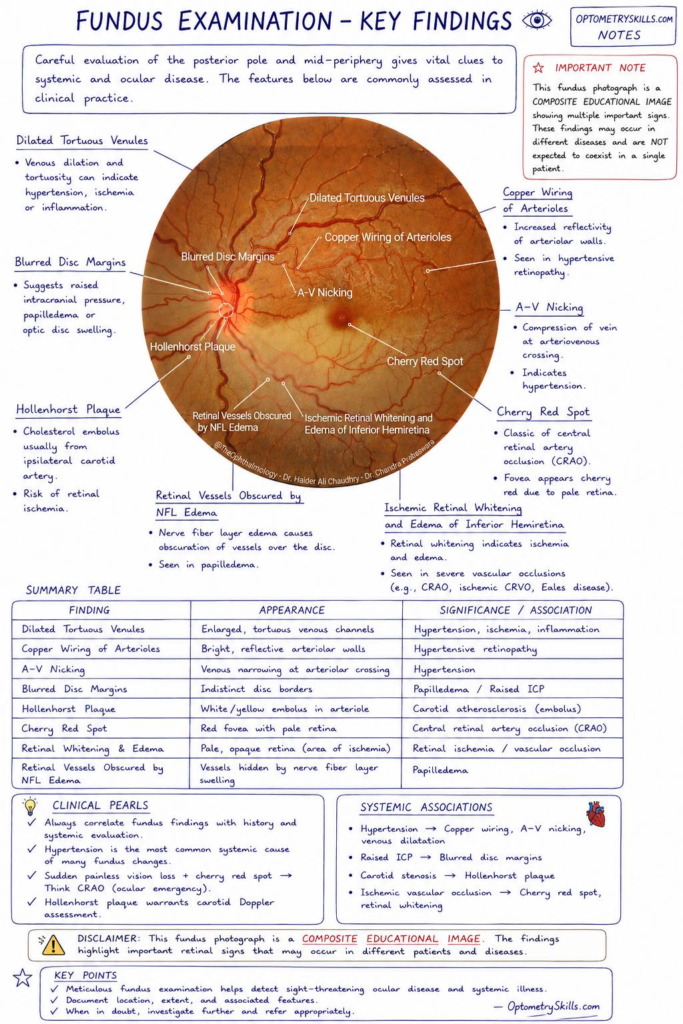
Mastering Fundus Examination: A Comprehensive Guide to Key Retinal Findings
by
Fahmina Jawed
May 12, 2026
This content is exclusively for our Facebook community members.
Login with Facebook
to access premium resources.