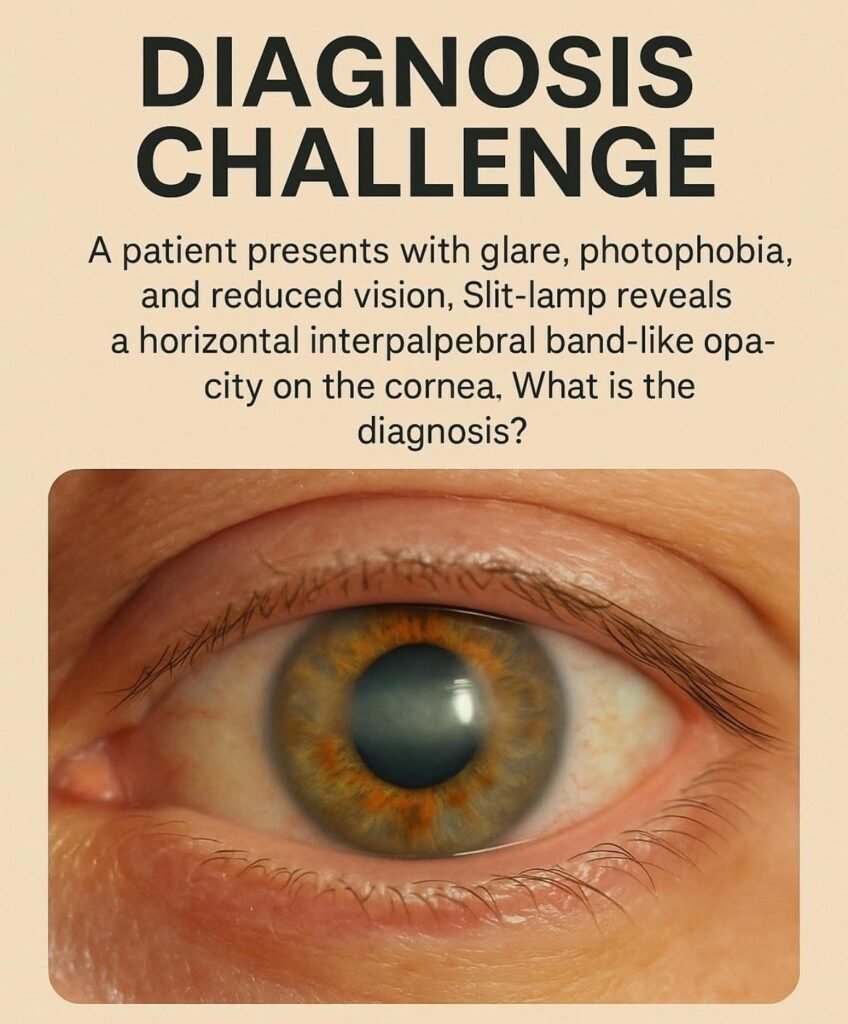
Calcific Band Keratopathy: Key Clinical Insights for Optometrists What is Calcific Band…
You must be a member to access this content.
View Membership Levels