
Honeycomb Corneal Epithelial Edema: Causes, Clinical Clues, and Management
Honeycomb corneal epithelial edema is a distinct form of corneal surface swelling characterized by a reticular or bullous epithelial pattern. Although it is relatively uncommon, its recognition is crucial in preventing misdiagnosis, particularly as it can resemble more serious pathologies such as herpetic keratitis or epithelial dystrophies. Honeycomb edema may arise from several underlying causes—most notably medication-induced effects—and usually resolves with appropriate management.
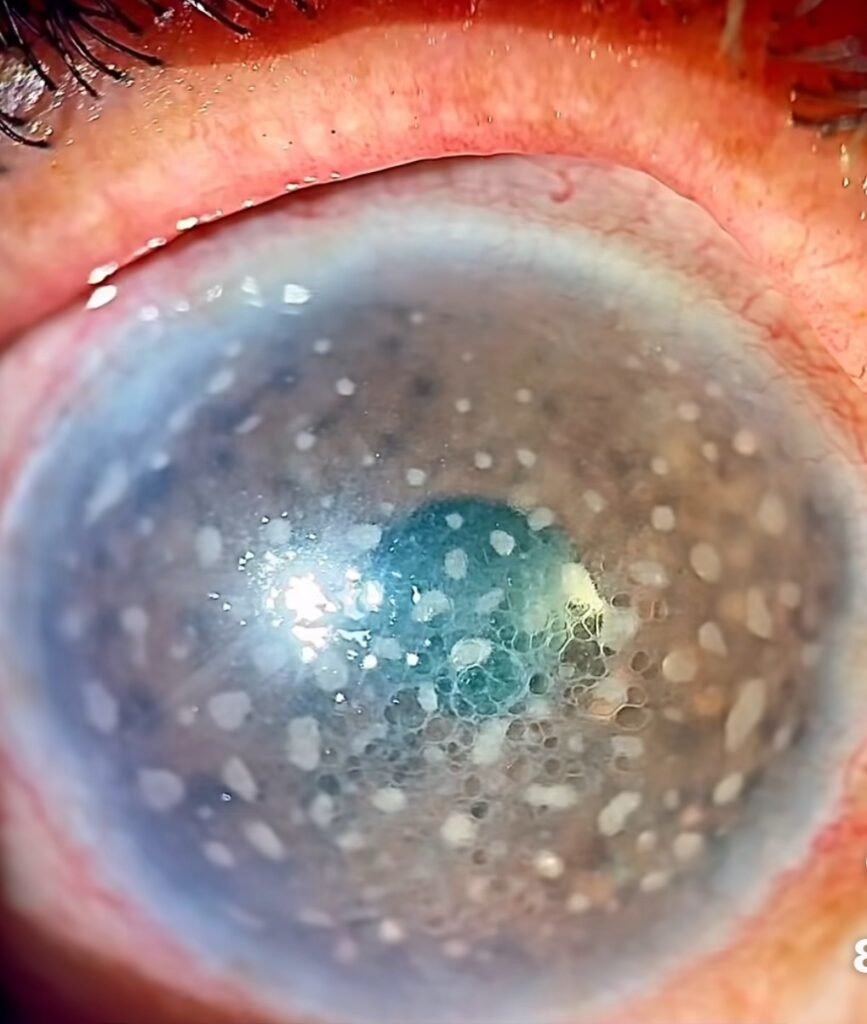
Picture credit- YepezRetinaCentre
Clinical Features
Honeycomb corneal edema presents as:
Small, clustered epithelial bullae in a reticular or net-like (“honeycomb”) pattern Most visible in the central or inferior cornea Minimal to no stromal involvement Best seen on slit-lamp with retroillumination or anterior segment OCT
Symptoms may include:
Blurred vision Mild foreign body sensation Photophobia Often asymptomatic in early cases
Causes of Honeycomb Corneal Epithelial Edema
1. Netarsudil (Rhopressa)
Netarsudil is a Rho-kinase inhibitor used to treat open-angle glaucoma and ocular hypertension. It is one of the most well-documented causes of honeycomb epithelial edema.
Mechanism: ROCK inhibition may alter corneal epithelial barrier function or interfere with fluid dynamics at the epithelial-stromal interface. Onset: Edema may develop within 1–3 weeks of starting therapy. Risk factors: Recent ocular surgery, pre-existing corneal endothelial dysfunction, or other glaucoma medications.
A 2020 case series (Wisely et al.) described 6 eyes developing reversible bullous epithelial edema after netarsudil, with resolution upon discontinuation.
2. Recent Ocular Surgery
Postoperative epithelial edema can develop in eyes after:
Cyclophotocoagulation Penetrating keratoplasty Cataract surgery, especially in the presence of compromised endothelium
Surgical trauma or inflammation can exacerbate epithelial barrier breakdown, particularly when combined with medications like netarsudil or prostaglandins.
3. Endothelial Dysfunction
Conditions like:
Fuchs endothelial corneal dystrophy (FECD) Chronic corneal decompensation can lead to microcystic epithelial edema, which may assume a honeycomb pattern in early stages.
4. Topical Medications or Toxic Keratopathy
Chronic use of: Preserved antiglaucoma medications (e.g., timolol, latanoprost with BAK) Topical anesthetics or NSAIDs can cause toxic epithelial damage manifesting as microbullous or reticular edema.
5. Elevated Intraocular Pressure
In rare cases, significant IOP spikes can lead to epithelial edema without stromal thickening, especially in young eyes. This edema may also assume a honeycomb configuration.
Honeycomb Corneal Epithelial Edema vs Keratic Precipitates
| Feature | Honeycomb Corneal Epithelial Edema | Keratic Precipitates (KPs) |
| Location | Epithelium (outermost corneal layer) | Endothelium (innermost corneal layer) |
| Appearance | Reticular or “honeycomb” pattern of small epithelial bullae | Whitish or pigmented granular deposits on the posterior cornea |
| Best Seen With | Slit-lamp (direct/retroillumination), anterior segment , OCT | Slit-lamp using specular reflection |
| Cause | Medication (e.g., netarsudil), post-op stress, epithelial dysfunction | Inflammation, usually uveitis (viral, autoimmune, TB, etc.) |
| Associated Symptoms | Mild blurring, foreign body sensation, usually no pain or redness | Pain, photophobia, redness, decreased vision |
| Pathophysiology | Fluid accumulation between/under epithelial cells | Inflammatory cells (macrophages, lymphocytes) sticking to endothelium |
| Resolution | Self-resolves after stopping the causative agent | Resolves with anti-inflammatory therapy (e.g., topical steroids) |
| Associated Findings | Normal anterior chamber, IOP may vary | Often accompanied by cells/flare in AC, synechiae, or hypopyon |
| Clinical Importance | May mimic herpetic or dystrophic patterns but is reversible | Suggests underlying uveitis or systemic inflammation |
Differential Diagnosis
Herpetic epithelial keratitis (usually dendritic/irregular, with terminal bulbs) Map-dot-fingerprint dystrophy Toxic keratopathy Microcystic edema due to endothelial failure
Careful history, medication review, and AS-OCT imaging help differentiate these conditions.
Management
🔹 Step 1: Identify and Eliminate the Cause
Discontinue netarsudil or other offending agents if implicated Stop any toxic drops or preservatives Treat elevated IOP if present
🔹 Step 2: Support Epithelial Recovery
Topical lubricants (non-preserved artificial tears) Hypertonic saline drops or ointments (e.g., 5% NaCl) to draw out fluid Bandage contact lenses (in symptomatic cases)
🔹 Step 3: Treat Underlying Conditions
Address ocular hypertension or glaucoma with alternative medications Monitor or refer for corneal endothelial assessment if FECD is suspected Manage postoperative inflammation and ensure adequate corneal hydration
🔹 Step 4: Follow-Up
Most cases resolve within 1–4 weeks once the trigger is removed Document resolution with serial photos or AS-OCT imaging Reassess medication choices to avoid recurrence
Prognosis
Excellent in most cases if identified early No long-term structural damage once edema resolves Recurrence is unlikely if causative agent is avoided
Conclusion
Honeycomb corneal epithelial edema is an important and recognizable clinical sign that often points toward netarsudil use or recent ocular procedures.
Early diagnosis and withdrawal of the inciting factor typically result in full resolution.
Eye care professionals should remain alert to this pattern, especially in glaucoma patients, to prevent misdiagnosis and ensure prompt management.
Bibliography & Further Reading
Wisely CE, et al. Reversible reticular epithelial corneal edema associated with netarsudil. Am J Ophthalmol Case Rep. 2020;17:100583. https://doi.org/10.1016/j.ajoc.2020.100583 Belovay GW, et al. Unilateral reticular epithelial edema associated with netarsudil use. Can J Ophthalmol. 2021;56(3):e95-e97. EyeWiki – Netarsudil-associated Corneal Epithelial Edema https://eyewiki.org/Netarsudil-associated_Corneal_Epithelial_Edema Sciencedirect Case Report on Honeycomb Edema https://www.sciencedirect.com/science/article/pii/S2451993622000330 Krachmer JH, Mannis MJ, Holland EJ. Cornea: Fundamentals, Diagnosis and Management. 4th ed. Elsevier; 2017.