
Understanding Corneal Pigmentations: Clinical Appearances and Diagnostic Insights
Corneal pigmentations are fascinating yet diagnostically significant findings in anterior segment examination. These pigment deposits can appear in various colors, patterns, and depths, often reflecting local pathology or systemic disease. For the clinician, the challenge lies in distinguishing benign, contact-lens–related pigmentation from those associated with conditions such as keratoconus, uveitis, or Wilson’s disease. This article summarizes the key corneal pigmentations every optometrist should recognize—highlighting their causes, appearance, and clinical implications.
Arlt’s Triangle
A brownish, triangular-shaped pigment deposit found inferiorly on the posterior cornea. It often indicates previous or chronic anterior uveitis, where inflammatory cells settle inferiorly due to gravity.
Brawny Edema
A brownish epithelial haze that suggests epithelial basement membrane dystrophy (EBMD) or recurrent corneal erosions. The edematous appearance reflects chronic epithelial compromise.
Ferry’s Line
An orange-brown ferric line formed around a surgical filtering bleb, commonly seen after glaucoma surgery. The line represents ferric ion deposition in the epithelium adjacent to the bleb.
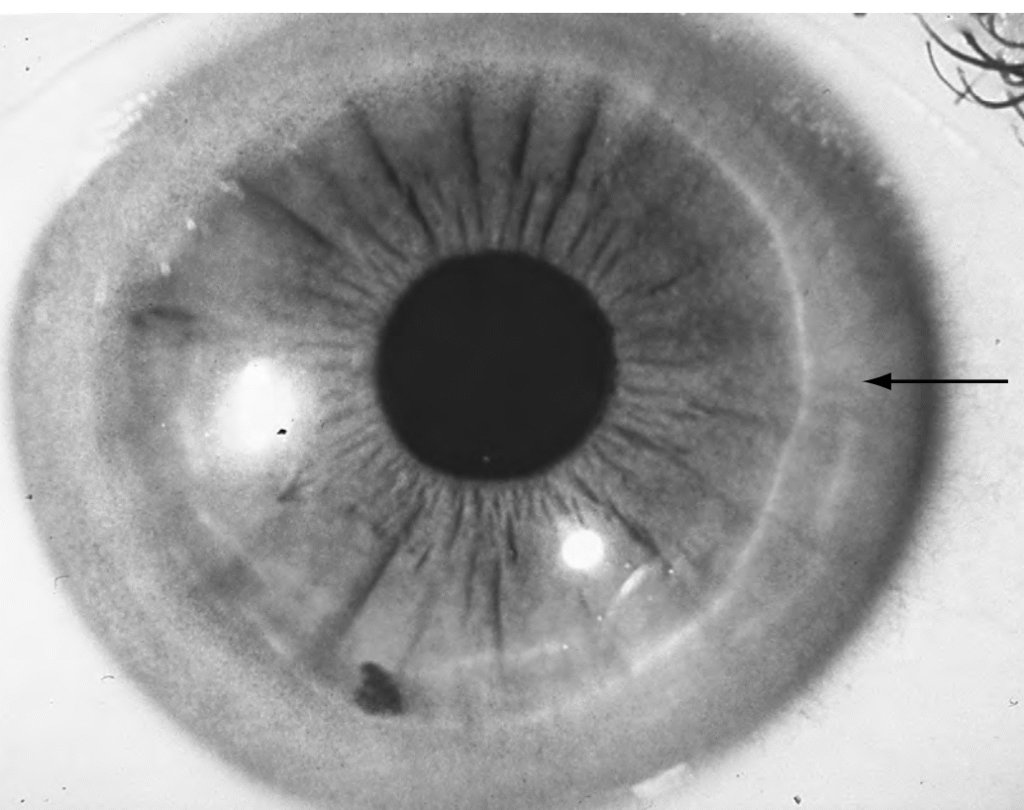
Fleischer’s Ring
A hallmark of keratoconus, this incomplete iron deposition occurs in the deep epithelium around the base of the corneal cone. It appears darker under cobalt blue light, enhancing visibility.
Goar’s Line
Consists of pigment granules forming a horizontal line on the inferior posterior cornea. Its presence is suggestive of pigmentary glaucoma and should prompt intraocular pressure monitoring.
Hemosiderosis
Represents intracorneal or posterior corneal blood staining, following neovascularization or hyphema. The brownish discoloration results from hemoglobin breakdown and iron accumulation within corneal tissue.
Hudson–Stähli Line
An orange-brown horizontal iron line at the epithelial basement membrane, usually in the middle third of the cornea. Common in older patients or previously injured corneas, it is typically benign and asymptomatic.
Kayser–Fleischer Ring
A golden-brown or greenish ring at the level of Descemet’s membrane due to copper deposition. It is characteristic of Wilson’s disease, a systemic disorder of copper metabolism.
Keratic Precipitates
White or pigmented deposits on the corneal endothelium indicating uveitis, trauma, or age-related endothelial changes. They may vary in size and pigmentation depending on the type and duration of inflammation.
Keratomelanocystosis
Appears as pigmented spokes radiating into the cornea from the limbus, typically at 4 and 8 o’clock. Seen predominantly in black patients, this finding may suggest trauma, infection, or toxic inflammation.
Krukenberg’s Spindle
A brown, vertical spindle-shaped pigment deposition on the posterior cornea. It results from dispersed iris pigment granules and is associated with pigment dispersion syndrome or old uveitis. Regular glaucoma monitoring is advised.
Melanin Deposition from Medications
Certain systemic drugs can cause corneal pigmentation. Phenothiazides produce fine stippling at Descemet’s membrane, chloroquine causes whorl-like opacities, and epinephrine can lead to adrenochrome deposition in Bowman’s layer. Trauma may also implant melanin deeper into the corneal epithelium.
Striate Melanokeratosis
Characterized by pigment-bearing cells extending from the limbus into the subepithelial cornea, forming streaks or whorl patterns. Common in black patients, it may develop after trauma, infection, or epithelial breakdown and tends to be permanent.
Salmon Patch
An orange-red stromal discoloration in interstitial keratitis, considered pathognomonic for syphilis. The coloration reflects inflammatory infiltration in the midstroma.
Sampaolesi’s Line
A pigment line deposited at Schwalbe’s line. Its presence is highly suggestive of pigmentary or pseudoexfoliation glaucoma, warranting further gonioscopic evaluation.
Stocker’s Line
A brownish ferric line at the leading edge of a pterygium, formed by iron deposition secondary to chronic tear flow alteration around the lesion.
Tattooing
Refers to variable corneal discoloration due to staining by heavy metals, drugs, or external pigments. Historically, corneal tattooing was used cosmetically or therapeutically to mask scars.
Vortex Keratopathy (Corneal Verticillata)
A whorl-like epithelial deposition pattern, typically centered in the lower cornea. It may be congenital and benign or acquired, commonly associated with Fabry’s disease or medications such as amiodarone, chloroquine, tamoxifen, suramin, and atovaquone. If systemic disease is suspected, α-galactosidase A enzyme assay can confirm Fabry’s disease. Infusion therapy may slow systemic progression, particularly renal complications.
Conclusion
Corneal pigmentations offer critical diagnostic clues, often serving as visible markers of deeper ocular or systemic disease. A detailed slit-lamp examination—with attention to color, location, pattern, and associated findings—helps clinicians distinguish benign physiological changes from pathology requiring intervention. Mastery of these subtle presentations enhances both diagnostic accuracy and patient care in anterior segment evaluation.